

When your face unexpectedly becomes numb, or begins to spasm, many HNPP sufferers do wonder what godforsaken cause could be behind it. Yet, it isn’t as uncommon as many may believe. Health professionals say that facial issues tend not to be associated with the condition, hence multitudes have been diagnosed with Bell’s Palsy instead.
What is Bell’s Palsy?
Bell’s palsy, or idiopathic facial paralysis (IFP), is the most common cause of unilateral, lower motor facial palsy. It’s origins remain uncertain. However, the first familial occurrence was found in 1887, hence hereditary factors have been considered to play a role in the etiology of the disease. It is believed to occur when the nerve that controls the muscles in your face becomes compressed and IFP is generally linked to inflammation or viral infections.
“In the last year and a half I have been dealing with one sided facial pain and numbness. It has evolved into a burning that sequentially involves the tongue, then lips, then cheek, then eye, then ear and finally throat all on the left side. It waxes and wanes and seems to do so based on my stress levels. I have had CT and MRI, normal; as well as a battery of blood tests, normal; seen a neurologist who said I’m fine (ahem!) and an ear nose and throat doc who says I have non-motor Bell’s Palsy (my research indicates there is no such thing).”
User on the BrainTalk Communities Forum
It’s obvious that there could be secondary condition causing facial issues, but several members of various HNPP groups have spoken about pain, weakness numbness, and spasms associated with the head and face.
Scientists have been studying the link between IFP and HNPP in order to get a better understanding of both causes. A letter in the Journal of Clinical Neuroscience in 2013 shows how the two conditions are not connected. Researchers at the Department of Neurology, Eginition Hospital, in Athens, Greece, hypothesised that a handful of participants in a study for Bell’s Palsy could have the same mutation for HNPP.
They say: “There are a few case reports of patients belonging to these subcategories of Bell’s palsy, on whom the characteristic deletion of a 1.5-Mb region on chromosome 17q11.2-12 which includes the peripheral myelin protein 22 (PMP22) gene, was detected.”
Out of a 145 unrelated Greek patients with Bell’s palsy, 28 patients with recurrent facial palsy and 18 patients with familial facial palsy were tested for a deletion of the PMP22 gene. However, none of the participants had this mutation.
“These cases could be part of a diverse spectrum of miscellaneous disorders including HNPP.”
“Is there a common genetic background?” Karadima, G. et al, 2013
They conclude: “Bell’s palsy seems to have a different etiology than HNPP. The same applies to familial or recurrent Bell’s palsy. A molecular genetic investigation for HNPP seems to be indicated in cases of recurrent or familial facial palsy accompanied by peripheral nervous system damage or exhibiting a family history of peripheral neuropathy. These cases could be part of a diverse spectrum of miscellaneous disorders including HNPP.”
This is reiterated in the 2009 case report Familial Recurrent Bell’s palsy conducted by researchers from the Department of Neurology, Zhejiang University, Hangzhou, China. Three families in which eight patients had a total of 12 episodes of typical Bell’s palsy were recorded in a bid to find the etiology of the condition.
In spite of this, the researchers infer: “Recurrent facial palsy can occur in neurological disorders such as Melkersson-Rosenthal syndrome (MRS), Moebius syndrome, Charcot-Marie-Tooth disease and hereditary neuropathy with liability to pressure palsy (HNPP). These conditions however, have additional features that distinguish them from idiopathic familials Bell’s palsy. None of our patients have any symptoms indicative of such diseases.”
So what’s the reasons behind facial numbness?
There are several possible causes of facial numbness, also known as hypesthesia. Most of these causes can be traced to a problem in or affecting the trigeminal nerve.
It is one of twelve cranial nerves and is one of the most widely distributed nerves in the head. The cranial nerves can be categorised as two main nerve types: those that control motor responses such as blinking, chewing, or eye muscle movement, and those that respond to the sensations of taste, smell, hearing, and touch.
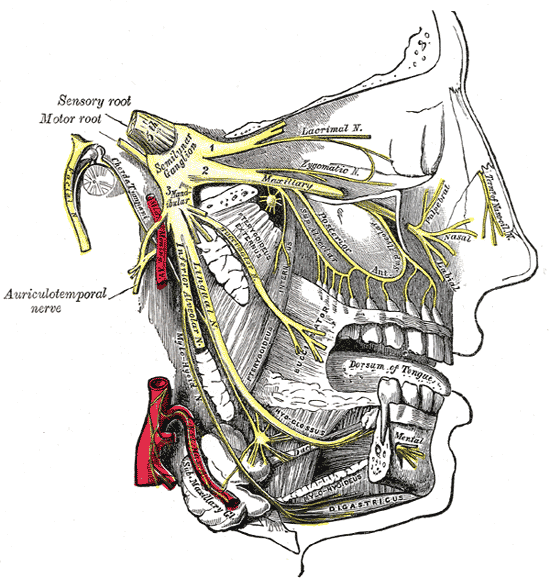
The trigeminal nerve has three branches, which controls both the sense of touch in areas in the face as well as the motor function associated with chewing. Damage to this nerve could, therefore, make chewing difficult, if not impossible. Some sufferers of face numbness also experience numb lips. Or it could create either a ‘pins and needles’ sensation or a loss of feeling in parts of the face. Of the twelve facial nerves, it is usually considered number five. Other parts affected include:
- Olfactory nerve (number 1) – relays the sense of smell to the brain.
- Oculomotor nerve (number 3) – controls the external muscles of the eye.
- Facial nerve (number 7) – controls the muscles used in facial expressions and should not be confused with the trigeminal nerve, despite its name. It does not relay a sense of touch.
- Auditory nerve (number 8) – controls balance and hearing.
While most of these are connected with the central nervous system, and HNPP is yet to have established links to the CNS, there have been cases where some with the condition have had issues with this particular nerve.
According to a 2015 study carried out by Japanese researchers from Department of Neurology, Osaka Red Cross Hospital, Osaka, there were two cases with cranial involvement without progressive muscular atrophy (PMA). They state: “a 40-year-old female case of HNPP with the involvement of the trigeminal, facial and hypoglossal nerves, and a case of 7-year-old boy having a homozygous deletion of PMP22, who had the LMN [lower motor neuron] impairment in the cranial nerves of VII and III, sensory disturbance in extremities.”
Like many other publications, the researchers state that because of limited studies, “additional investigations are warranted to better understand PMP22 regulation in the CNS and the peripheral nervous system”.
The rarity of such finding is highlighted in a Brazilian study from the Department of Neuroscience at the University of São Paulo. In the 2016 study Clinical and Neurophysiological Features of HNPP, 39 patients were reviewed for neurological symptoms while 33 were given nerve conduction tests. Only one presented cranial nerve related symptoms in terms of “involvement of the trigeminal nerve and other one an episodic involvement of the eyelid branch of the oculomotor nerve”.
They go on to restate: “Cranial nerve involvement was rare in our population […] It seems that this is the pattern in most studies Interestingly, we have previously described a HNPP patient that developed dysphagia. Other rare manifestations in our patients were pes cavus and nerve thickening, as seems to be the case in most studies.”
In the 2006 book Differential Diagnosis in Neurology by Robert J. Schwartzman, MD, the Professor of Neurology documents daily morning reports with neurology residents and the examination of patients in front of colleagues over the last 30 years. The Emeritus Professor of Neurology at the Drexel University College of Medicine in Philadelphia, recounts that “facial nerve involvement occurs rarely” with HNPP.
Therefore, it’s important to realise the symptoms instead of the condition as knowing that it is HNPP, or in this case, may not be HNPP-related, does not change the fact that these symptoms are manifesting.
For many with facial issues, including those suffering from HNPP, it’s vital to get it checked by a medical professional as it could be associated with another underlying or even acute disorder. In many situations, doctors may dismiss it as HNPP and then resort to medication associated with the inherited disorder, because they aren’t certain of what it may be, which is where your persistence to get the correct treatment will be absolutely key.
