If you didn’t think it was possible, but some individuals with HNPP claim they suffer from breathing problems due to anomalies with certain nerves. Breathing problems associated with hereditary neuropathy are often ignored because most doctors don’t know they can be part of the disorder.
While hyperventilation is less common, weakness of the thoracic diaphragm, which enables people to breathe, and the nerve linked to it is suggested to cause problems with breathing.
Disclaimer: Please ask your medical practitioner or doctor for more information. This article is based on various research, journals and testimonies.
Why does it happen?
HNPP makes the nerves very susceptible to trauma, which plays a pivotal role when it comes to the act of inhaling and exhaling. There are several major issues that create specific problems:
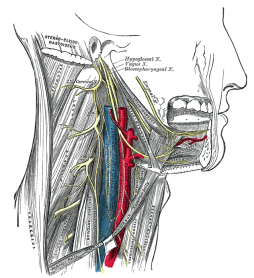
Hypoglossal Nerve
The hypoglossal nerve is the twelfth paired nerve in the brain. Its name is derived from ancient Greek, ‘hypo‘ meaning under, and ‘glossal’ meaning tongue. The nerve has a purely somatic motor function, innervating the majority of the muscles of the tongue.
According to the 2015 study Disorders of the Lower Cranial Nerves by authors Josef Finsterer and Wolfgang Grisold, the nerve directs not only voluntary activities of the tongue, but also involuntary functions, such as clearing the mouth of saliva by swallowing. They report that some people with HNPP have been reported to have issues with this specific nerve. The authors state: “Another [lower cranial nerve] involved in HNPP is the hypoglossal nerve. The affection of the hypoglossal nerve has been also reported in other types of hereditary neuropathy.”
Researchers at the Department of Neurobiology, Tokyo Metropolitan Institute for Neuroscience, say that there is a distinct link between swallowing and breathing. Using six rats, they report: “The XII nerve activity preceding that of the phrenic nerve (pre-I XII nerve activity) was markedly exaggerated during periods when this relation was disrupted”.
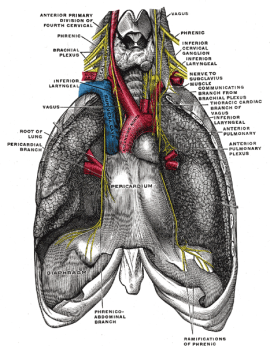
The phrenic nerve plays an important role in breathing because the nerve originates in the neck passes down between the lung and heart to reach the diaphragm. It is responsible for controlling the contractions of the diaphragm, which allows the lungs to take in and release air and make us breathe properly. During the above experiment with the rats, the authors say that “nerve activity was also shown to couple with swallowing in the same manner as ‘real’ inspiratory activity.”
You may experience this when your breath arrests for a moment while attempting to swallow, which brings me neatly on to the significance of the phrenic nerve.
Phrenic Nerve
Nerve fibres of the phrenic nerve, spinal nerves, and laryngeus recurrens nerve project to the diaphragm, abdominal, intercostal, and laryngeal muscles. While it is considered “exceptional”, some HNPP sufferers do face these symptoms.
In the 2016 report Laryngeal and Phrenic Nerve Involvement in a Patient with Hereditary Neuropathy with Liability to Pressure Palsies, the participant is said to have had vocal cord paralysis as well as “latency of the right phrenic nerve” and reduced right hemi-diaphragm – the muscle that separates the chest cavity from the abdomen and that serves as the main muscle of respiration.
The study suggests that a person with comorbidity, or someone who suffers from several separate illnesses which in this case was chronic obstructive pulmonary disease (COPD), can consequently end up with breathing issues. They also say that this was rectified through COPD treatment. Potential weight loss from HNPP could be a triggering factor.
This video by Professor Mary Reilly from the National Hospital for Neurology in London, UK, explains breathing issues for those suffering from the inherited condition Charcot Marie-Tooth syndrome:
Brachial plexopathy can be an issue withh HNPP sufferers. It is a form of peripheral neuropathy which occurs when there is damage to the brachial plexus, an area on each side of the neck where nerve roots from the spinal cord split into each arm’s nerves. Nerves outside the brachial plexus, extends from the spinal cord, through the cervicoaxillary canal in the neck, over the first rib, and into the armpit.
The phrenic nerve receives stimuli from parts of both the cervical plexus and the brachial plexus of nerves. As Satish Khadilkar and Snehaldatta Khade state in the Official Journal of Indian Academy of Neurology: “Hereditary neuropathy with pressure palsies can present phenotypically like acute brachial plexopathy. But, unlike the classical phenotype, recurrence is unusual.”
Hence damage to this area could potentially weaken signals and cause breathing difficulties.
How likely is it occur?
However, it’s important to note that respiratory issues are more common with the inherited condition Charcot Marie-Tooth syndrome. In a 2016 study including 49 patients with genetically confirmed CMT or HNPP, those with a duplication of the PMP22 gene as well as those with a mutation of the MPZ gene were more likely to face issues with breathing. The HNPP participants were recorded not to have faced respiratory problems.
The authors of Underestimated Associated Features in CMT Neuropathies say that those with the CMT2-I/J (Charcot Marie-Tooth syndrome Type 2) condition had certain mutations in the MPZ gene causing “respiratory insufficiency”, which obviously reiterates the rarity of this occurring when a person suffers from HNPP.
This video, made by CMTA, explains what’s going on in more detail:
The organisation CMT UK has recommended the following, which may be applicable to those with HNPP if you feel that you are suffering from breathing issues.
What to do if you think you’re having breathing difficulties
- Have your doctor send you to a cardio-pulmonary specialist for a sleep study.
- Suggest that your maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP) be tested both sitting and lying down.
- If you are having bad morning headaches you could be retaining CO2. The above tests will show that.
- You can elevate the head (from the waist) of your bed two or three inches by putting bricks under the legs or a suitcase under the mattress.
- You can keep your weight down.
- Make sure you have had a pneumonia and flu vaccinations (ask your GP) and treat respiratory infections aggressively.
As mentioned, breathing problems is rather a rare symptom to be associated with HNPP. That being said, there is still a lot of research to be undertaken to establish other symptoms associated with the condition. The main thing is not to hold back and visit your medical practitioner if you feel there may be a problem.